How ACOs Should Approach FWA Campaigns: The Case for Structured Outreach
by Yubin Park, Co-Founder / CTO
Every ACO has a fraud, waste, and abuse problem. Most just don't know the shape of it.
Medicare recorded $54.3 billion in improper payments in FY2024. That number is useful for scale. But the category-level spikes are what should concern ACOs most — because they show how fast a billing anomaly can grow before formal enforcement catches up.
Two recent examples make this concrete. Medicare spending on urinary catheter codes A4352 and A4353 jumped from $153 million in 2021 to $3.1 billion in 2023 — roughly 20x in two years. The surge was so disruptive that CMS issued a final rule to retroactively exclude those codes from CY2023 ACO financial calculations. ACOs were being penalized for spending they had no ability to control. Skin substitutes followed a similar arc — Medicare Part B spending grew from roughly $256 million in 2019 to over $10 billion by 2024, prompting a major OIG report citing serious FWA concerns and enforcement actions totaling over a billion dollars in recoveries.
The common thread: both categories ballooned for months before regulators responded. By the time charges were filed or payment policy changed, the money had already left the system. ACOs that waited for external intervention absorbed the losses.
Claims data flows in continuously. NCD/LCD guidelines define what CMS will pay for. And somewhere in between, billing irregularities accumulate — quietly, at scale, without triggering any alert. By the time a MAC review surfaces a pattern, months of unnecessary spend have already passed.
There's a better approach. And it's producing measurable results today.
The Signal Is Already in Your Claims Data
National and Local Coverage Determinations (NCD/LCD) are the coverage policies that govern what Medicare will pay for. They specify which diagnoses justify a procedure, what documentation is required, and when a service is medically necessary. Every billing provider is expected to follow them.
When a claim doesn't meet NCD/LCD criteria, that's not automatically fraud. It may be a documentation gap, a coding error, or an outdated billing practice. But at scale, systematic deviations from these guidelines are a signal worth investigating.
This is where ACO claims data becomes a powerful asset. An ACO with attributed populations across hundreds of providers can identify which providers are consistently billing outside coverage guidelines — and at what dollar value. The pattern that would take a MAC review cycle months to surface can emerge from your own data in days.
Top tip
NCD/LCD guidelines vary by MAC jurisdiction and are updated regularly. A provider billing correctly last year may be out of compliance today. Educational outreach often resolves what looks like a compliance issue but is really an awareness gap.
How Sentinel Surfaces These Cases
Falcon's Sentinel product is built for systematic claims analysis. It applies proprietary algorithms against ACO claims data, cross-referencing flagged claims against applicable NCD/LCD guidelines and enriching the analysis with broader datasets — claims history, provider benchmarks, utilization patterns, and national billing norms. We've written about the data pillars that make this kind of analysis possible.
The output isn't a list of suspected fraudsters. It's a prioritized case set: providers whose billing patterns appear inconsistent with coverage determinations, ranked by anomaly strength and potential dollar impact. Each case includes the specific claims, the relevant policy, and the nature of the deviation — giving your team a clear, defensible basis for outreach.
Then Sentinel does something most analytics tools don't: it generates the outreach letters.
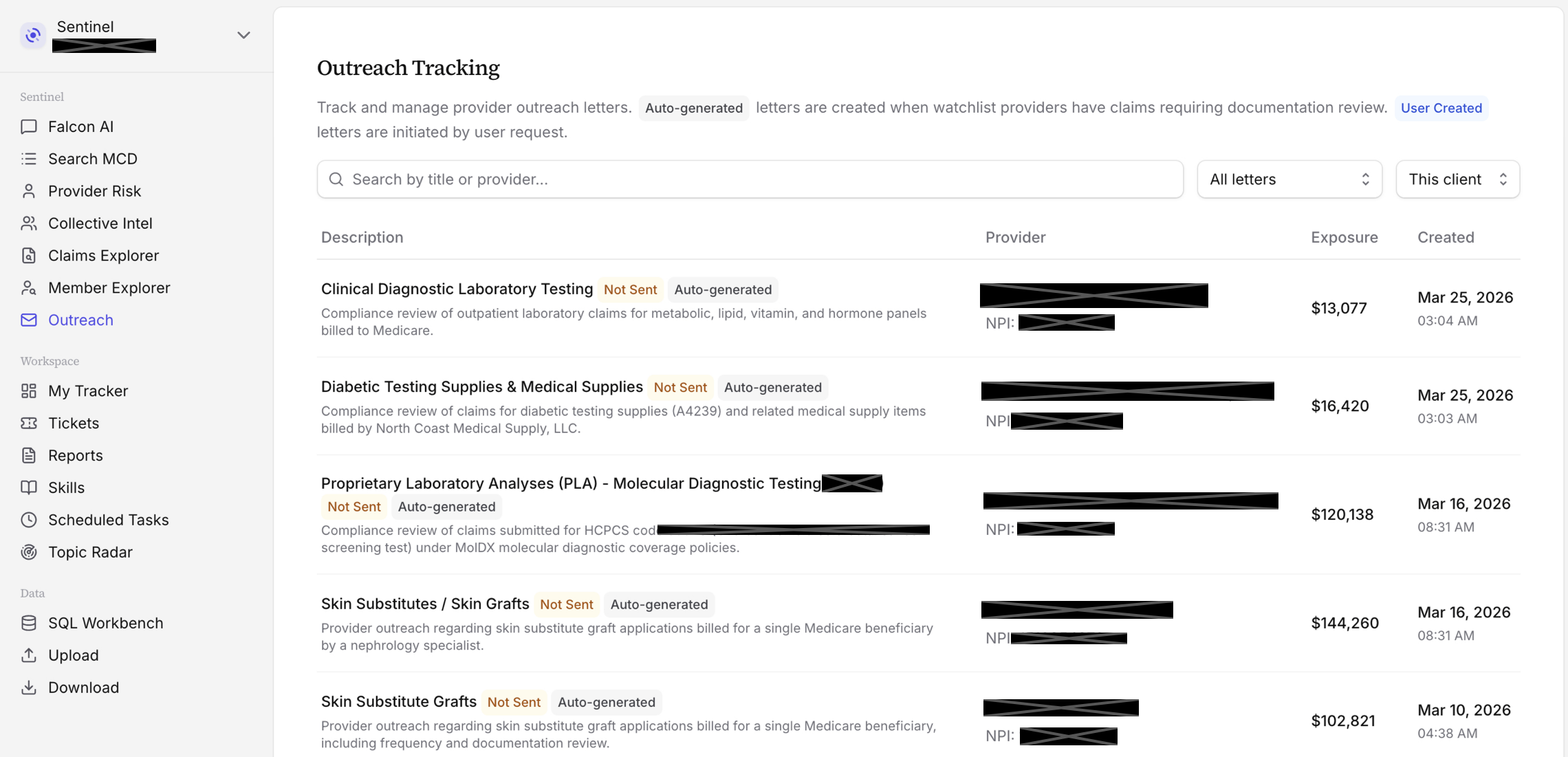
The screenshot above shows the Outreach Tracking queue inside Sentinel. Each row is a case — a provider, a category of concern (laboratory testing, skin substitutes, DME supplies, etc.), and the total claims exposure in dollars. Letters marked "Auto-generated" were drafted by the system based on the flagged claims; "User Created" ones were initiated by your team directly. Both types go through the same review-and-send workflow.
Each letter is calibrated to the specific case. It presents the identified anomaly, cites the applicable NCD/LCD, and requests clinical justification for the claims in question. The tone is educational, not accusatory. Providers get a specific, evidence-based inquiry — not a vague documentation request. They have a clear opportunity to respond, clarify, or self-correct.
Your team reviews and approves every letter before it goes out. The platform tracks status end to end: sent, responded, resolved, escalated.
Why Educational Outreach Works
Honestly, we weren't sure what to expect. ACOs needed to do something with the findings — sitting on flagged claims wasn't an option. So we sent letters. The results were surprising.
A significant share of providers voluntarily reversed claims and returned funds. Looking back, it makes sense. Most billing irregularities aren't sophisticated fraud. They're compliance failures: outdated billing practices, documentation that doesn't match what was coded, misapplication of a coverage guideline that changed. When a provider receives a specific letter pointing to a discrete set of claims and asking for clinical justification, many will review their records, find they can't support the billing, and reverse the claims.
The letter works because it presents something formal enforcement rarely does: a concrete question about a specific set of claims, with the evidence attached. It's harder to ignore than a general audit inquiry. And because it comes from the ACO rather than a MAC or OIG, it carries a professional relationship dynamic that formal enforcement lacks.
Top tip
Providers who self-correct after outreach rarely repeat the same pattern. A single targeted letter often resolves not just the flagged claims but the underlying billing practice — with effects on future claims that don't show up in the initial recovery calculation.
Speed matters too. Formal MAC referrals can take twelve to eighteen months to produce any resolution. Educational outreach letters often produce responses within weeks. Recoveries happen in the current period, not after an extended adjudication cycle.
The Results
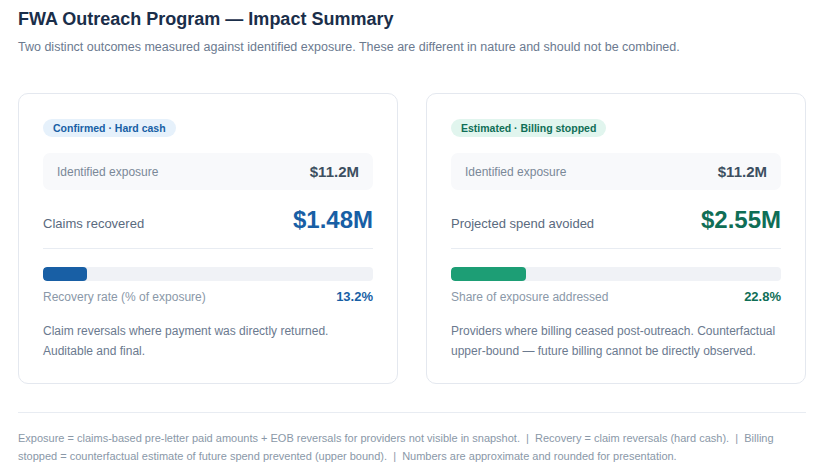
The impact summary above tracks two distinct outcomes — and it's important not to combine them.
The left panel, Confirmed — Hard Cash, captures claim reversals where payment was directly returned. These numbers are auditable and final. This is real money back.
The right panel, Estimated — Billing Stopped, captures something harder to measure: providers who stopped the problematic billing pattern after outreach. The spend avoided is a counterfactual estimate — future billing can't be directly observed, so this is an upper bound, not a guarantee.
The dollar figures shown are masked for client confidentiality, but the structure and relative trends are consistent across our ACO clients. The key ratios to focus on: roughly 13% of identified exposure converts to hard cash recovery, while another ~23% of exposure is addressed through billing cessation. Taken together, more than a third of flagged exposure gets resolved — without any formal enforcement action.
Recoveries have ranged from hundreds of thousands to several million dollars per ACO depending on ACO size and volume of flagged billings. The ACOs seeing the largest recoveries are the ones running campaigns systematically — not as one-off reviews, but as a regular process integrated into their compliance workflows.
Structured Campaigns, Not One-Off Reviews
The difference between ACOs that see significant recovery and those that don't usually comes down to process. A one-off analysis produces a list. A structured campaign produces a workflow — flagging, letter generation, tracking, follow-up, escalation — that runs continuously and compounds over time.
The economics are straightforward. The cost of running Sentinel is fixed. The return scales with the volume of cases surfaced. ACOs that treat FWA analytics as a standing program capture more recovery, build institutional knowledge about their high-risk provider segments, and maintain a documented compliance posture that holds up under scrutiny.
The providers most likely to self-correct are also the ones most likely to respond to professional, evidence-based outreach. Formal enforcement remains the right tool for cases where it's warranted. But for the large proportion of billing irregularities that represent correctable compliance failures, it's a slow tool for a problem that can be resolved much faster.
If you're an ACO that hasn't run a systematic NCD/LCD compliance analysis, the recoveries are likely there waiting. Get in touch to see what Sentinel surfaces in your population.