Research Brief: Anomalous Urinary Catheter Billing and the ACO Exposure
by Yubin Park, Co-Founder / CTO
White Paper · Research Brief #1
This page summarizes the brief. The full 12-page white paper — including methodology, figures, and supplier-level findings — is available as a PDF.
Read the Full White Paper (PDF)
This is the first installment in Falcon's Research Brief series — short white papers documenting specific anomalous billing patterns we surface across ACO claims data, the regulatory context around them, and what they mean for organizations bearing the financial risk.
The opening brief examines urinary catheter codes A4352 and A4353. Medicare spending on these two codes climbed from roughly $153 million in 2021 to $3.1 billion in 2023 — close to a 20x increase in two years. The surge was severe enough that CMS issued a final rule retroactively excluding the codes from CY2023 ACO financial calculations. ACOs were being penalized for spending they had no realistic ability to control.
This is the pattern that makes ACOs uniquely vulnerable. The bad actors driving these spikes do not bill the ACO directly — they bill Medicare, often through DME suppliers operating well outside an ACO's attributed provider network. But because attributed beneficiaries receive the supplies, the spend lands inside the ACO's total cost of care. ACOs become the financial target of activity they neither generated nor authorized, and the lag between the billing surge and any regulatory response is measured in months or years, not days.
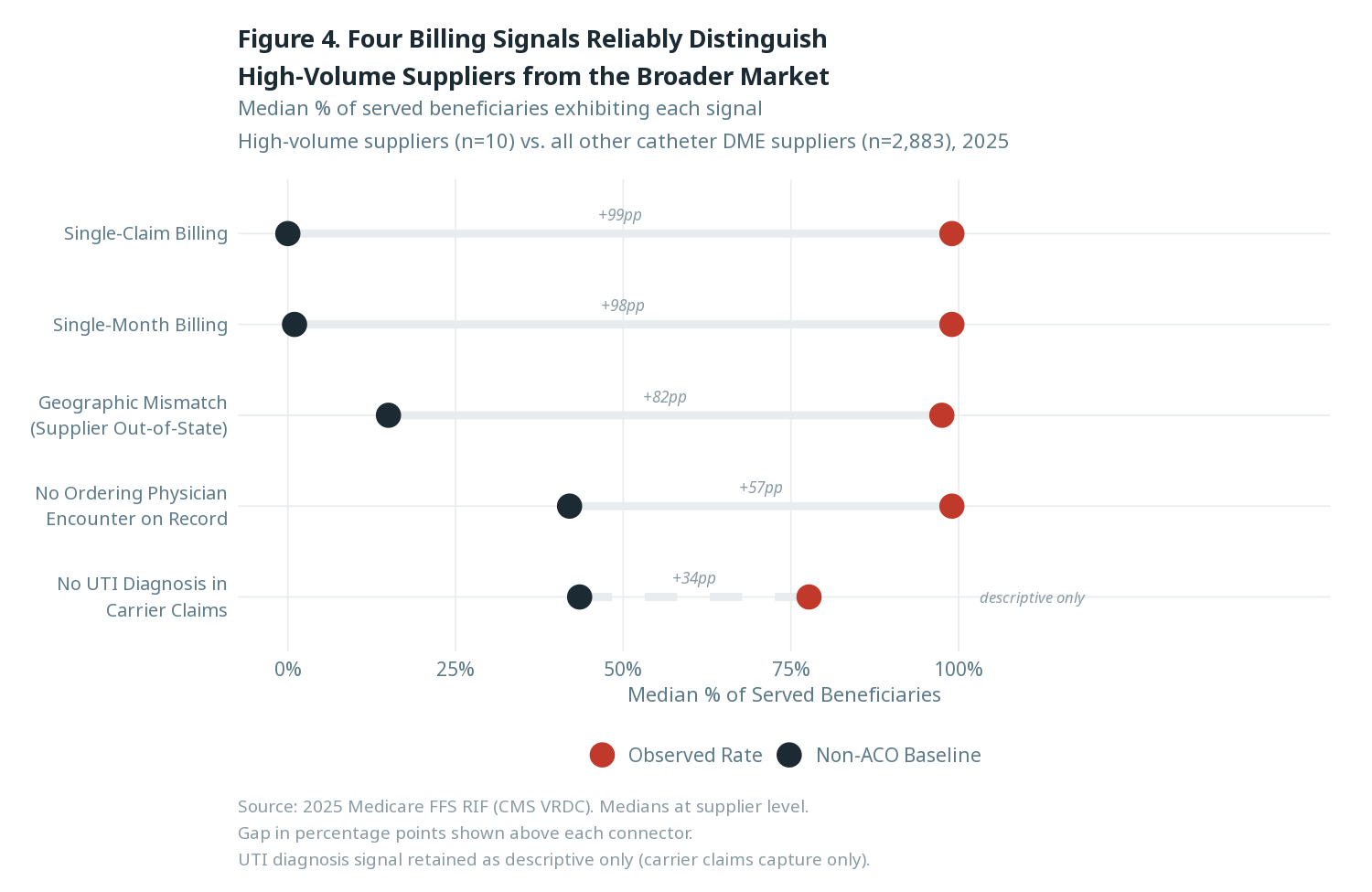
The full brief walks through the timeline of the catheter anomaly, the regulatory response, and the implications for ACO compliance and FWA programs. Inside, we identify four billing signals that reliably separate the small set of high-volume catheter suppliers driving the anomaly from the broader DME market — a sample of which is shown below.
Read the full white paper for the complete analysis. If you'd like to discuss what similar patterns may exist in your own attributed population, get in touch.